|
Your standard blood panel was built to flag disease. It was not built to predict the next twenty years.
A "normal" result on the panel you got at your last physical means your numbers fell inside a population reference range. The reference range was constructed from millions of people, most of them not optimising for healthspan. Normal is the average of sick. Optimal is the line you actually want.
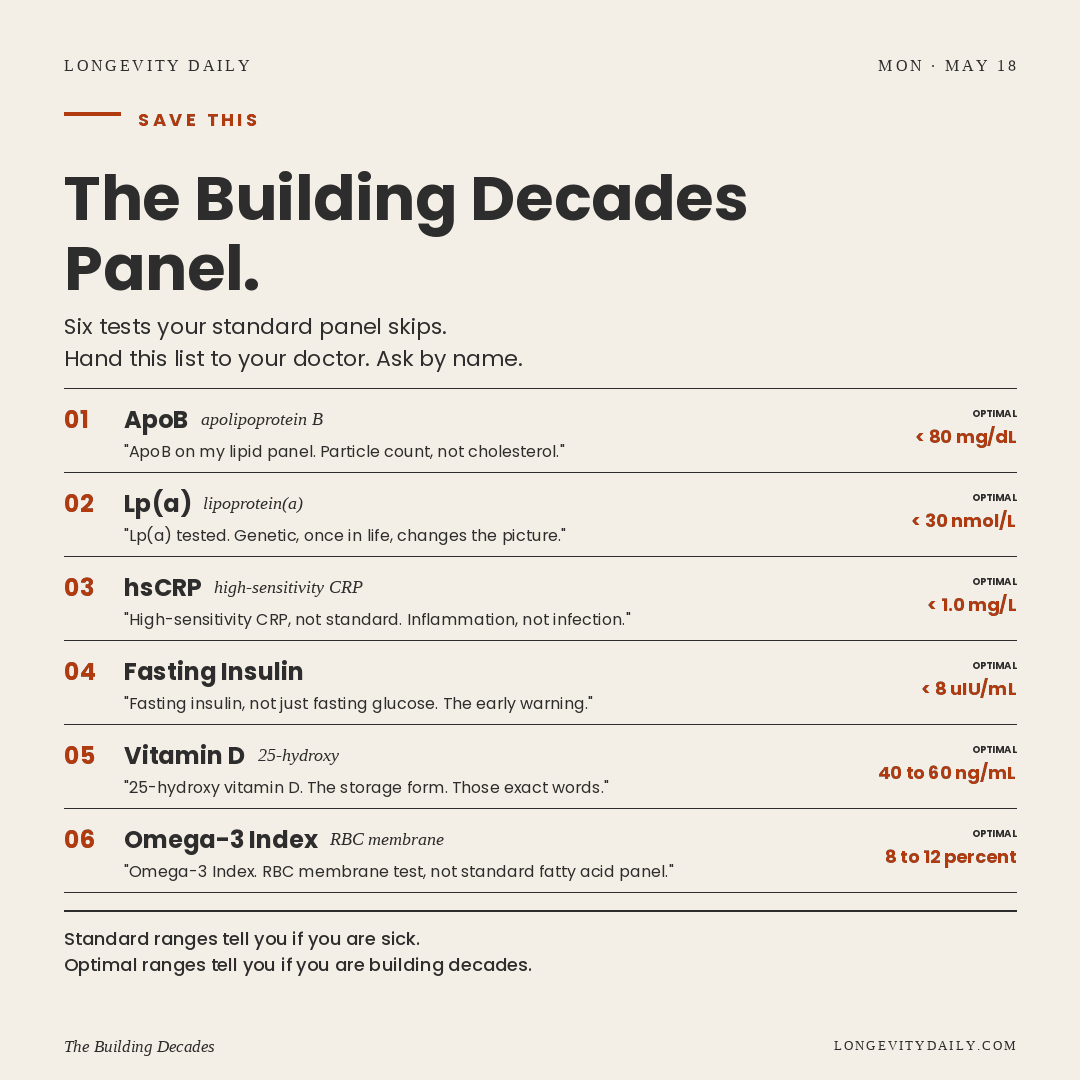
There are six tests that, taken together, predict cardiovascular, metabolic, and inflammatory risk in midlife more accurately than the standard panel ever will. Most aren't ordered unless you ask, by name. The script is in our Blood Work Cheat Sheet at the bottom of this email. Use it.
|
|
ApoB, apolipoprotein B, is the protein every atherogenic particle in your blood carries exactly one of. The largest analysis to date, Sniderman et al, JAMA Cardiology 2019 (n=398,718), showed ApoB outperformed both LDL-C and non-HDL-C as a predictor of cardiovascular events. The European Atherosclerosis Society now treats it as the preferred marker. It does not appear on a standard lipid panel. Optimal sits below 80 mg/dL. Most adults under 45 have never had it measured.
Fasting insulin is the earliest metabolic warning signal you can buy. Glucose and HbA1c lag insulin by years. A 2017 meta-analysis in Bioscience Reports (Zhang et al) found each unit rise in fasting insulin, even within the standard "normal" range, correlated with a 5 percent increase in cardiovascular risk. In absolute terms, that compounds: an insulin of 15 versus optimal 6 shifts a healthy 45-year-old's 10-year cardiovascular risk from roughly 6 percent into the 9 percent range. Most labs don't flag concern until 24.9 uIU/mL, three to five times higher than longevity-clinic optimal. Optimal: under 8 uIU/mL.
High-sensitivity CRP measures the chronic, smouldering inflammation that drives cardiovascular, metabolic, and neurodegenerative disease over decades. The JUPITER trial, Ridker et al, NEJM 2008 (n=17,802), showed that lowering inflammation, with no change in cholesterol, cut major cardiovascular events. Above 3.0 mg/L roughly doubles heart attack risk: against a baseline 10-year MI rate of around 4 percent in a healthy 45-year-old, that's a shift from 4 percent to about 8 percent. JUPITER's number needed to treat to prevent one event over five years was 25. Below 1.0 mg/L is where you want to live. Standard CRP, the version your doctor might order, only catches acute infection. Ask for the high-sensitivity version, by those exact words.
|
Standard reference ranges tell you if you are sick. Optimal ranges tell you if you are building decades.
|
Lp(a) is the cardiovascular risk most people have never been tested for. It is 80 to 90 percent genetic, set largely at birth, and not meaningfully movable with diet, exercise, or statins. The 2022 European Atherosclerosis Society Consensus on Lp(a), Kronenberg et al, European Heart Journal pooled the global data: elevated Lp(a) carries roughly two-to-four-fold cardiovascular risk depending on threshold. In absolute terms, that pushes a baseline 10-year cardiovascular event rate of around 5 percent into the 10 to 20 percent range, before any other risk factor is counted. Lp(a) affects roughly 20 percent of the global population. You only need it tested once in your life. Optimal: under 30 nmol/L.
Vitamin D, measured as 25-hydroxy vitamin D, is the storage form that reflects your actual reserves. A 2014 meta-analysis in BMJ (Chowdhury et al, n=849,412) found vitamin D deficiency was associated with a 35 percent increased risk of cardiovascular death. In absolute terms, for a midlife adult, that moves 10-year cardiovascular mortality from roughly 4 percent to around 5.4 percent. Over 40 percent of adults globally are insufficient. Optimal sits at 40 to 60 ng/mL. Most standard panels do not include it. Ask for the 25-hydroxy form, by name.
The Omega-3 Index measures the EPA and DHA percentage in your red blood cell membranes, not a single-moment fatty acid reading. It is the most reliable long-term marker of omega-3 status. The Harris and Von Schacky framework, Preventive Medicine 2004 and subsequent work showed an index below 4 percent associates with the highest risk of sudden cardiac death, and 8 to 12 percent associates with a roughly 30 percent reduction in cardiovascular mortality. In absolute terms, that 30 percent reduction translates to about 1.2 percentage points of 10-year cardiovascular mortality for a midlife adult, or one death prevented per roughly 80 people who move from a 4 percent index up into the 8 percent range. Most Western adults sit at 3 to 5 percent. Standard panels do not test it. Some labs offer it as an add-on; some require an out-of-pocket request.
That is six tests. Together they answer the questions the standard panel does not: how many atherogenic particles are circulating, how reactive the arterial wall, how genetically loaded the dice, how nutrient-replete the system. The advanced panel costs roughly $150 to $250 out of pocket if your insurance does not cover all six. It buys you a decade of clarity.
|
|
The first conversation is the hardest. Most clinicians will not push back if you ask by name. If your doctor declines a specific test, you can order an advanced panel directly through a service like Ulta Lab Tests or Function Health; the six combined run $150 to $250. Lp(a) only needs to be tested once. Everything else gets retested every six to twelve months under 50, every six over.
Once the numbers are in, the action is unglamorous. Mediterranean-style diet, daily zone 2 cardio, strength training twice weekly, seven to eight hours of sleep, sunlight, omega-3-rich fish or supplementation, low alcohol. Most of these markers move within three to six months. Sleep matters more than most people realise here. Poor sleep measurably worsens lipid profiles, inflammation, and insulin, often within a single bad week.
If you are over 40 and have never had an advanced panel, do it once. The Blood Work Cheat Sheet at the link below carries the full ten markers, three ranges each, and the exact script to hand to your doctor.
|